







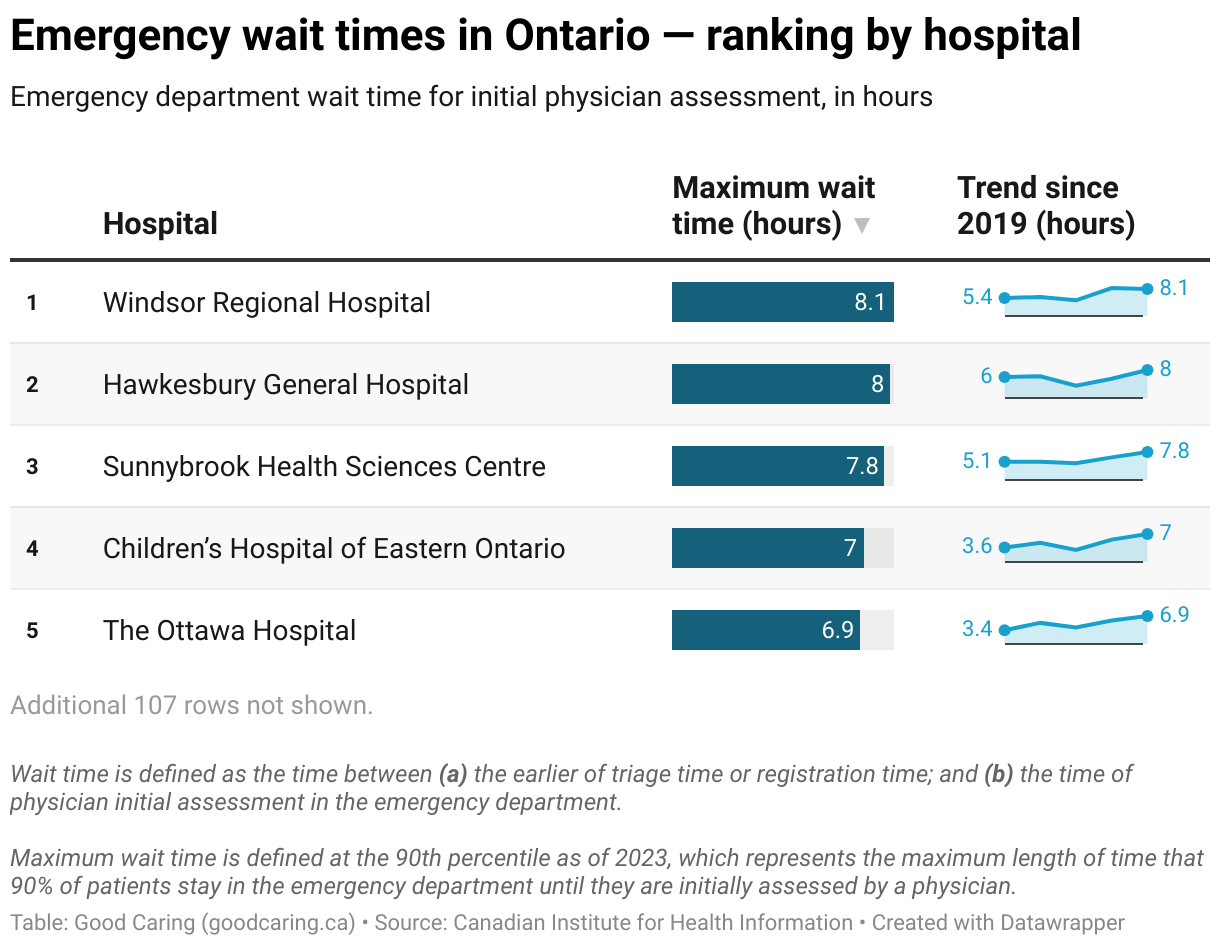
In the northeast corner of Toronto, Sunnybrook Health Sciences Centre rises from a sprawling campus of modern glass towers and low-slung brick buildings. It is part hospital, part research hub, and part trauma response center. Sunnybrook handles more than 1.2 million patient visits annually, serving not only its surrounding neighborhoods but also much of Ontario. It functions as both a local lifeline and a specialized destination for the province’s most critical cases.
Its emergency department embodies the strain of that dual role. Designed for rapid, high-turnover care, it now absorbs some of the most complex and delayed cases in the system. Patients lie on stretchers in hallways. Wait times stretch from minutes to hours, and sometimes longer. Behind the congestion are deeper system tensions—workforce limitations, care access gaps, and structural demands that emergency rooms were never built to carry.
Institutional Growth and Spatial Limits
Sunnybrook opened in 1948 as a veterans’ hospital. Over the decades, it evolved into one of Canada’s most advanced academic health centers. It now houses regional programs in trauma, neurology, oncology, cardiovascular medicine, and geriatrics. Yet despite its expanding mission, the hospital’s emergency department remains confined by its older physical design.
The current emergency layout reflects earlier assumptions about emergency medicine—limited complexity, short stays, and predictable patient flow. But today, Sunnybrook’s emergency department must accommodate not only high volume but also high-acuity and long-duration cases. It faces physical constraints that limit its flexibility, even as the hospital’s regional referrals and local demand both intensify.
Urban Pressure and Demographic Change
The hospital sits at the edge of North York, one of Toronto’s fastest-growing districts. The area’s population continues to rise, shaped by urban densification, aging, and immigration. Sunnybrook’s local catchment area now includes some of the city’s most demographically diverse and densely populated neighborhoods.
Older adults account for a growing share of emergency visits. These patients often arrive with multiple conditions, requiring more complex and prolonged assessments. Meanwhile, younger patients seek care for mental health crises, injuries, or unmanaged chronic disease. With limited alternatives during evenings and weekends, many residents turn to the emergency department as a default option for urgent care.
Every new residential development adds pressure to the hospital’s front doors. In dense urban pockets like Don Mills and Leaside, high-rises and retirement homes bring in more patients who often lack regular access to primary care. This intensifies the demand on emergency services already stretched thin.
Access Gaps in Community-Based Care
Toronto has a strong network of healthcare providers, but access remains uneven. Many patients near Sunnybrook lack timely access to family doctors or after-hours clinics. For them, the emergency department becomes a primary point of contact with the health system.
Mental health stands out as a persistent pressure point. Emergency staff regularly encounter cases involving anxiety, depression, suicidal ideation, and substance use. Although Sunnybrook maintains a psychiatric assessment unit, it has limited capacity. Delays in mental health evaluations result in patients staying in emergency spaces for extended periods, occupying beds that could be used for incoming cases.
Patients with chronic illnesses, such as heart failure or diabetes, often return due to unstable outpatient management. Gaps in medication access or follow-up care mean that emergency visits are sometimes preventable but still frequent. These cases take longer to assess and treat, reducing the department’s overall throughput.
Social and Economic Pressures
The region around Sunnybrook is economically mixed. It includes some of Toronto’s most affluent enclaves but also pockets of poverty, precarious housing, and food insecurity. These conditions affect how and when people seek care.
Patients with unstable housing or financial stress may delay medical attention until symptoms become severe. Others use the emergency department for all health needs, given difficulties navigating or affording other parts of the system. Homelessness, now more visible across Toronto, contributes to recurring visits and prolonged stays for issues that could often be managed with adequate social support.
Housing instability also affects discharge planning. Patients ready to leave the hospital may have no safe place to recover, increasing the likelihood of re-admission and prolonging their emergency stay.
Cultural and Linguistic Complexity
North York is among the most linguistically diverse areas in Canada. Patients at Sunnybrook speak a wide range of languages, and their cultural expectations for care can vary widely.
Interpreter services are available but often overbooked. In their absence, communication can break down, delaying diagnosis and treatment. Differences in how pain is described, how mental illness is understood, or how families participate in care decisions all contribute to potential misalignment between staff and patients.
Emergency department staff must quickly interpret not only symptoms but also social cues. In high-pressure settings, this adds another layer of complexity. Even with ongoing cultural competency training, the pace and volume of cases make consistent application difficult.
The Weight of Specialized Responsibility
Sunnybrook is Ontario’s largest trauma center and one of only two adult Level 1 trauma centers in the Greater Toronto Area. It is also a referral center for complex stroke and burn cases. As such, it regularly receives patients from other hospitals by ambulance or helicopter.
These arrivals cannot be deferred. When a trauma or stroke alert comes in, resources must be mobilized immediately, regardless of the department’s current occupancy. This often forces delays for less acute patients already waiting. The department must remain prepared for sudden influxes, which may upend carefully planned workflows.
These responsibilities create tension between its regional mandate and its local obligations. A resident with a minor injury may wait while teams focus on a complex trauma case from another city. This balancing act reflects the hospital’s broad role, but also its vulnerability to unexpected surges.
Workforce Pressures
Staffing is another major constraint. Physician coverage remains relatively stable, but nursing shortages persist. Many shifts run without full complement, limiting the number of patients who can be safely managed at once.
Emergency nurses at Sunnybrook must be prepared for any scenario—mass casualty events, mental health crises, pediatric codes, or geriatric emergencies. This constant vigilance, paired with overcrowding, takes a toll. Burnout rates are rising, and turnover undermines institutional knowledge.
Other departments also affect emergency flow. Delays in laboratory results or diagnostic imaging slow down decision-making. Limited availability of porters, housekeeping staff, and diagnostic technicians creates further friction in patient movement. When one link in the chain falters, the entire system slows.
Backlogs in Testing and Admissions
Many patients in Sunnybrook’s emergency department are not waiting for evaluation—they are waiting for diagnostic tests or inpatient beds. Advanced imaging services such as computed tomography or magnetic resonance imaging are in constant use. Even with 24-hour access, demand often exceeds supply.
Once a decision to admit is made, another delay begins. Inpatient beds are frequently unavailable, particularly for specialized services such as neurology or cardiac care. Patients remain in emergency bays for hours or even days, monitored by emergency staff instead of transitioning to the appropriate inpatient team.
This phenomenon, known as boarding, strains emergency operations. Stretchers are occupied, staff are overextended, and the department’s capacity to accept new patients is reduced.
Systemic Factors and Provincial Policy
The situation at Sunnybrook reflects province-wide challenges. Many emergency departments across Ontario face rising volumes, especially during flu season or viral outbreaks. Community-based programs designed to alleviate emergency burden have expanded, but their integration remains uneven.
Efforts to improve care coordination—through home care, virtual visits, or urgent care clinics—have yielded mixed results. Many programs remain underfunded or lack strong ties to hospitals. In practice, emergency departments still absorb the overflow from gaps elsewhere in the system.
Delays in long-term care placements and rehabilitation discharges also affect Sunnybrook. Patients who no longer require acute care remain in beds for extended periods, limiting availability for new admissions from the emergency department. This creates a cascade of delays that begins long before the patient arrives at the hospital.
Funding mechanisms add further complexity. Hospital budgets are often based on local demographics, not on actual patient acuity or volume. As a provincial center, Sunnybrook carries a load that exceeds what its funding formulas account for. Infrastructure and workforce investments have not kept pace with demand.
Incremental Responses and Innovation
Despite these challenges, Sunnybrook has introduced several strategies to improve emergency flow. It has adopted rapid triage systems and embedded social workers into the department. Pilot projects involving virtual consultations aim to redirect low-acuity cases before they arrive at the hospital.
The hospital is also experimenting with artificial intelligence tools to predict patient volume and acuity. These models could support dynamic staffing decisions and better resource allocation, although they are still in development and require careful integration with existing systems.
Partnerships with community agencies have expanded. For frequent emergency users, case managers now coordinate follow-up care, mental health services, and housing supports. These efforts have shown early promise in reducing avoidable visits.
Toward Structural Change
Improving emergency wait times at Sunnybrook will require more than workflow tweaks or technological fixes. The department’s challenges are deeply connected to broader health system pressures. Without changes in how Ontario funds, staffs, and coordinates care, emergency departments will continue to function as the system’s catch-all.
Community-based services must become more accessible and better integrated. Investments in mental health, housing, and long-term care will help prevent emergencies before they begin. Policy must reflect the dual role of institutions like Sunnybrook, and funding must follow the actual demands placed upon them.
Staff must also be supported. This means not only adequate staffing ratios, but also long-term career pathways, mental health supports, and workplace stability. Retaining experienced nurses and technicians is as critical as recruiting new ones.
Conclusion
At Sunnybrook Health Sciences Centre, emergency department wait times are not just a matter of minutes or hours—they are a symptom of broader system stress. The hospital continues to serve its dual mission as a community provider and regional lifeline. But doing so under current conditions is becoming unsustainable.
Patients keep arriving. Ambulances keep coming. Helicopters keep landing. And behind each stretcher is a story—not only of illness or injury, but of a system that no longer moves fast enough to meet its own standards.
Sunnybrook’s emergency department stands at the convergence of expertise, pressure, and resilience. It is doing more than it was ever designed to do. But the question is no longer how much it can bear. The question now is how long it can continue without something giving way.







