







North York General Hospital, a cornerstone of Toronto’s healthcare system, is often lauded for its operational excellence. Recognized as one of the top community academic hospitals in Canada, it stands as a critical access point for acute care, diagnostics, surgery, and specialized medicine in the city’s north end. But within the sleek corridors of its bustling emergency department, the reality mirrors a more sobering truth—rising demand, long wait times, and system-wide pressures that increasingly defy even the most efficient practices.
Serving a population of more than 400,000 residents in neighborhoods like Don Mills, Willowdale, and Bayview Village, the hospital’s emergency department is one of the busiest in the city. It operates around the clock, every day of the year, and handles a mix of trauma, mental health crises, pediatric cases, and chronic disease flare-ups. Staff are seasoned. The hospital is well managed. But the volumes keep growing, and the space keeps tightening.
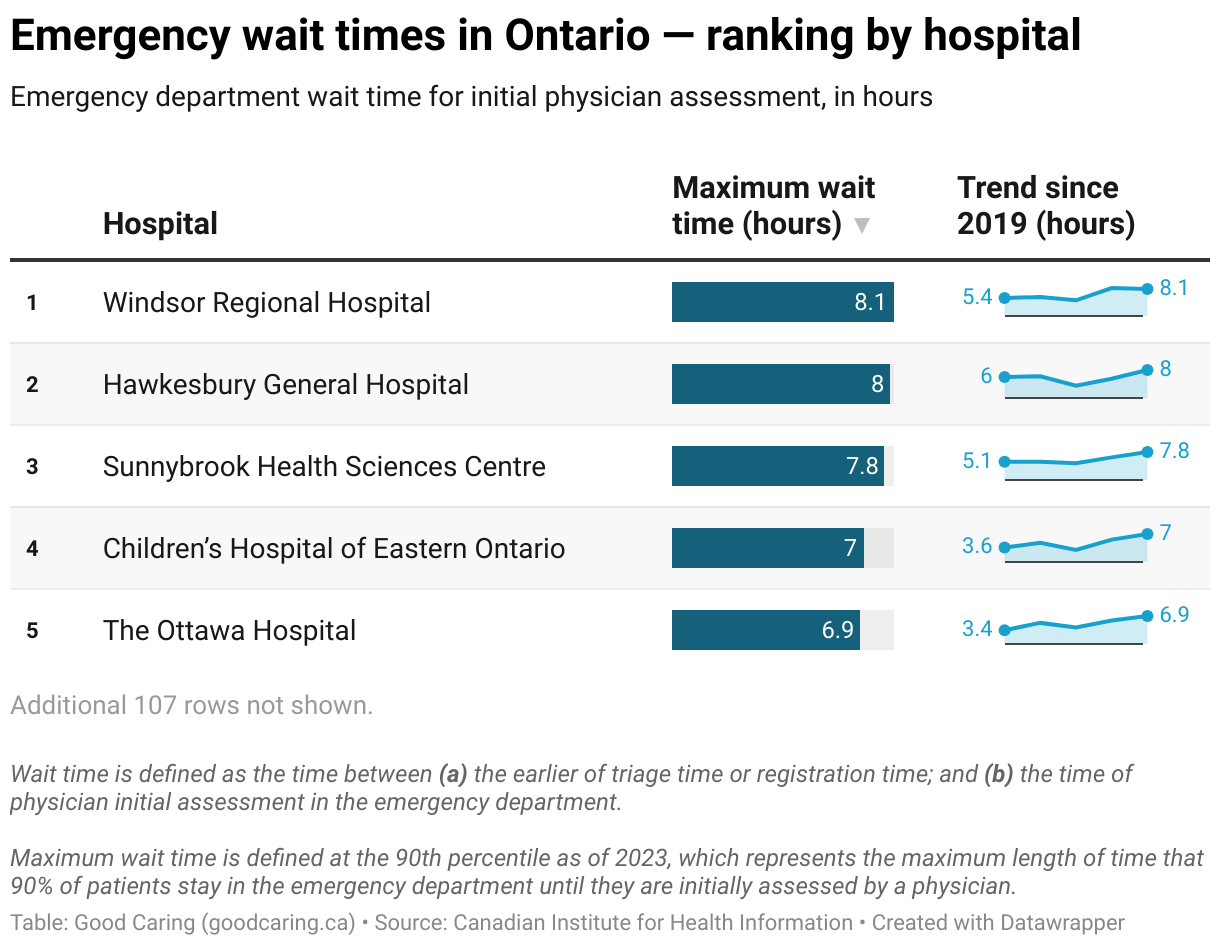
Emergency departments across Ontario are straining. At North York General, those strains are highly visible. Patients wait in lineups that stretch into the early morning. Ambulance offloads are delayed. Hallways become treatment zones. Staff speak of burnout in cautious, professional tones. And the hospital’s performance, once a model of efficiency, is now being weighed down by systemic deficits it cannot fix alone.
A Community Anchor with Regional Reach
North York General opened its doors in 1968 as a regional medical center for the city’s growing suburbs. Today, it’s a full-service, academic-affiliated hospital with over 400 beds, extensive outpatient services, and a teaching partnership with the University of Toronto. It is known for its surgical programs, maternal care, cancer treatment, and geriatric services.
The emergency department sees approximately 110,000 visits annually—more than many urban tertiary centers. It operates as a hybrid community and referral hospital, serving local residents while also absorbing overflow from surrounding facilities. It is connected to the broader Toronto hospital system but distinct in its role as a high-volume community access point with academic capability.
Its catchment area includes newly developed high-rise corridors and aging suburban neighborhoods. The demographic mix is complex: affluent homeowners, new immigrants, long-time renters, and seniors aging in place. Each patient group brings unique needs—and all converge at the emergency entrance.
Growth, Demographics, and Demand
Toronto’s population continues to climb, and the neighborhoods served by North York General are among the most dynamic. Condominiums and mixed-use developments have multiplied along major corridors like Sheppard and Yonge. With them come new families, international students, and seniors downsizing from larger homes.
This growth brings demand—not just in volume but in complexity. Young families present with pediatric emergencies. Older adults arrive with complications of chronic illness. New immigrants may be navigating the health system for the first time. Others come from long-term care homes, where staff rely on the emergency department for after-hours medical support.
Seniors now make up a growing share of emergency department visits. Many arrive with multiple comorbidities: dementia, heart failure, kidney disease. Their care requires longer assessment, more testing, and more coordination. Some are admitted. Others are held in emergency, waiting for upstairs beds that remain full.
Primary Care Erosion
One of the most significant contributors to emergency congestion at North York General is the erosion of timely access to primary care. Many patients who arrive at the hospital could, in theory, be managed in a clinic. But the system around them has eroded.
Family doctors in Toronto are retiring faster than they’re being replaced. Walk-in clinics are overwhelmed. Urgent care centers are few and far between. Patients report waiting days or weeks for appointments—or being turned away entirely.
For those with chronic conditions, missed follow-up leads to deterioration. For new immigrants, language barriers, housing instability, and lack of documentation complicate access. For working families, irregular hours and transportation limits make emergency the only feasible option.
The emergency department at North York General becomes the point of last resort. And each non-urgent case adds to a growing line that slows triage and delays care for those in genuine medical crisis.
Chronic Disease and Repeat Visits
Patients with unmanaged or poorly controlled chronic conditions frequently return to the emergency department. Heart failure exacerbations, poorly controlled diabetes, and respiratory issues often stem from missed follow-ups, medication nonadherence, or social barriers to care.
Many of these visits are preventable. But without adequate home care, chronic disease management, or outpatient coordination, patients default to emergency care. This recurring pattern contributes to overall volume and limits availability for acute emergencies.
North York General has developed strategies to flag high-frequency users and connect them with case managers or community partners. However, these efforts are resource intensive and cannot fully offset the broader system gaps that drive repeat emergency use.
Boarding and Delayed Transfers
Boarding—the practice of holding admitted patients in emergency due to lack of inpatient beds—is perhaps the most direct cause of emergency congestion at North York General. On any given shift, a significant portion of emergency space is occupied by patients who are no longer emergency cases but have nowhere else to go.
These patients require medication, food, monitoring, and communication with inpatient teams. They take up stretchers that could be used for triage. Their presence slows turnover, reduces capacity, and creates bottlenecks.
The reasons for boarding are systemic. Inpatient units are full. Discharges are delayed by a lack of home care, rehabilitation beds, or long-term care placement. Complex patients with no fixed address or inadequate support remain stuck in hospital—blocking flow from emergency to ward.
Diagnostic Bottlenecks and Throughput
Even when patients are seen promptly, diagnostic delays contribute to long stays. Blood tests, X-rays, ultrasounds, and CT scans are often backlogged. Consultations from specialists may take hours. Discharge can be delayed by a single pending test.
The hospital has invested in modern diagnostics, but demand exceeds capacity. Overnight, imaging availability decreases. Staffing thins. And a single complex case can stall the entire flow.
Infrastructure is modern—but still constrained. The emergency department was not built for its current volume. Privacy is limited. Stretchers overflow. Staff work in tight spaces. Renovations help—but do not replace the need for systemic reform.
Staffing Realities and Operational Strain
North York General’s emergency department has a reputation for well-managed operations. But it remains subject to the same staffing pressures facing hospitals across Ontario. Nurse vacancies, shift shortfalls, and burnout are ongoing concerns.
Emergency nurses face physical and emotional demands with each shift. They are often the first point of contact for patients in pain, distress, or confusion. Fatigue affects morale and retention. Junior nurses are trained quickly but require time to build the experience needed in high-acuity environments.
Physician workloads have also intensified. Patient complexity and administrative responsibilities leave little room for recovery. Shift work is constant, and leadership responsibilities often fall to the same core group of staff.
Operational excellence can stretch resources far—but not indefinitely. North York General continues to innovate around scheduling, onboarding, and team-based care. Yet, the human capacity of the department remains finite.
Community Partnerships and Innovation
Despite the challenges, North York General has pursued proactive strategies to manage demand. It operates rapid assessment zones to quickly process low-acuity cases. Nurse practitioner-led teams help divert patients from full emergency workups. The hospital partners with community health centers to ensure smoother discharge transitions.
Social workers and interpreters are embedded within the emergency department to address socioeconomic and linguistic barriers. The hospital also participates in research around predictive modeling and virtual care to anticipate and redirect potential surges in emergency visits.
These programs improve care quality and patient satisfaction. They also reflect the hospital’s commitment to innovation. However, even the most efficient programs cannot overcome foundational access gaps elsewhere in the health system.
Conclusion
North York General Hospital continues to deliver high-quality emergency care under increasingly difficult conditions. Its emergency department embodies both the strengths and the vulnerabilities of Ontario’s healthcare system. Operational strength and staff dedication have kept it afloat—but not immune to the strains seen across the province.
The rising demand, aging population, delayed discharges, and primary care access gaps converge in the emergency space. For every patient who leaves satisfied, another waits longer than they should. The margin for resilience is narrowing.
If the province is serious about reducing emergency wait times, it must look beyond the emergency doors. Solutions lie in upstream investment—in primary care, long-term care, diagnostics, and staffing. Until then, departments like North York General’s will keep absorbing the pressure, doing more than they were built to handle.
They are not overwhelmed because they are failing. They are overwhelmed because they are succeeding—under conditions that make success harder each day.







